
August blog
General Practitioners
In 1948, chose NOT to be employed by the State, (like NHS Dentists) but to remain
as self-employed “contractors”
Initially, each GP owned their own premises, many partnership GPs still do.
It takes straight As, five years hard graft at Medical school, plus four years
hospital training to be accredited.
Doctors and Dentists used to get free tuition, but now end up with £100k
debt.
In training, they have to pay exam fees etc, and like JDs, rent a house.
If their “business” has huge debts, they can go bankrupt, and many
“hand in” (quit) their NHS contracts and CLOSE.
There are 2000 fewer GPs, each with increased numbers of patients 1900 to 2300
If their staff deserve and are awarded a 6% rise, and their gas, electric bills rise 8%, their income (the remainder) falls.
They see 37 patients a day, work 7.30am to 7.30pm, and many are burnout, exhausted and dangerous.
They have been coerced into employing PAs-the ARRS funding DOES reimburse theses
salaries
but NOT additional GPs-which ARRS does not…
If they use PAs, their risk of losing GMC registration is increased, their workload doubled-as they are supposed to re-examine, re-history, recheck every quack PA consult face to face.
Many take the best way out-retire early, cut their hours. Some have anxiety, depression, alcohol problems, abuse wives, divorce…
Last year, government pegged funding rise to 1.9%!!!!!!!
Each patient attracts only £160 for all consults over a year-unlimited consults, not risen for years....
The government regards Doctors as “the enemy”, rather than cooperate,
listen, take on board their constructive ideas.
The right wing rags like The Telegraph, The Mail, The Times-print hate stories
about GPs
and politicians regularly describe them as “lazy, work-shy, part timers,
immensely rich, avaricious and greedy...
Doctors Association UK YouTube video briefing to MPs
Doctors Association UK website
There are not enough GPs. Their training places are blocked in preference for PAs-Politician's Apologies.
Partnerships cannot use ARRS funding to hire more GPs, only PAs...
As emergency measure-for one ytear only-GPs CAN hire GPs
but through Primary Care Networks-one GP shared accross several practices...
GPs want certainty and control of their health centres-GPs funded in core contract.
Since 2015 lost 2,000 GPs
Funding since 2015 reduced by 10-12%
GP wages for staff, Agenda f Change were 6%
Bills increased by 6%
Funding is pegged at 1.9%
Many practices CLOSED in last twelve months...
20% MORE appointments per day cf 2019
Each doctor is paid £159.61 per patient-no matter how many consults

Junior Doctors, Resident Doctors will vote on a pay restoration:
22.3% over two years-over two years, no restoration of 35%
Yousesef El-Gingihy wrote about the recurring battles between right wing, "shrink the state" governments and the NHS frontline medical workfporce
He even foresaw the introduction of PAs, AAs to dilute the real medics and beat the BMA!!!
The Junior Doctor's strike was an example of these recurring battles to end the NHS
Hunt communicated with Murdoch in the BSkyB row-and recruited Murdock to "win"
All the usual phrases came out again:
The NHS is broken
JDs are lazy, only concerned about their wages
Tony Blair's advice
"Anything nasty-do it in the first few months-the electorate will have forgotten about it at the next election..."
 ...
...
Every move was to get more work for less pay, no matter what the poor quality
Weekend comprehensive operating would be possible with more correctly paid staff, operating theatres and teams,
but NOT with then current workforce, salaries and restraint investment...
neoliberal right wingers like
Tufton Street think tanks
IEA
Governments-both Tory under Hunt, Javid,
and Labour under Streeting
want PAs, AAs
Community hubs-stuffed with PAs (like Operose "practices"), "supervised" ?remotely? by one real GP...
end the real NHS by UnAccountable Care Organisations (aka DisIntegrated Care Systems) allowed to keep profits after minimal care
Kaiser Permanente-reduce hospital costs by offloading onto underfunded GPs
https://lowdownnhs.info
The Lowdown and Keep Our NHS Public
The Lowdown NHS campaign group, Keep Our NHS Public: well researched, well-argued support for a publicly owned, publicly run NHS and Social Care, especially John Lister
The whole strategy recently has been to
-overpower and dilute real Doctors and the British Medical Association
-bribe the General Medical Council , the Royal College of Physicians, NHSEngland
have all been coerced, bribed to comply and promote PAs and AAs.
-to fool patients into believing the are seeing a real Doctor or Anaesthetist...
to make NHS care cheaper-not better...
Wes Streeting-very dangerous man
Darzi-previous reccomendations disaster
Penny Dash-McKinsey privatiser, marketiser
Managers only keep their jobs if they belive in marketisation, privatisation, throughput, balance the books by cuts
https://lowdownnhs.info/news/dash-in-to-take-charge-in-nw-london/
https://lowdownnhs.info/comment/opposition-to-north-west-london-experiment-is-still-growing/
Community
Hubs-not GP surgeries
Quoted here-because this strategy is so damaging and important... by the excellent John Lister
A bizarre experiment is being acted out in North West London. Its Integrated
Care Board, covering the third largest population of all 42 ICBs in England
was discovered at the end of January to be embarking on a scheme to fundamentally
change primary care services by April 1 – with no plan for consultation
with GPs, patients or the wider public.
Their plan was a root and branch reorganisation that would replace the role
of GP practices in handling calls seeking a same-day consultation. Instead of
practice staff passing calls on to their GPs, North West London’s boroughs
would be carved up into a smaller number of “hubs,” each covering
one or more of the 45 Primary Care Networks.
According to the ICB’s model, hub call handlers would divert almost all
calls (93 percent) to staff other than GPs, leaving a token GP to “supervise”
the handling of calls – and speak to the remaining 7 percent of patients.
The role of the GP in each hub would be reduced to call centre supervisor, with
other GPs left dealing only with complex cases and chronic sick and non-urgent
care.
Had some of the confidential documents outlining the scheme not been “leaked”
into the right hands, many GPs and their patients would have been effectively
faced with an ambush, with little chance to resist.
That was clearly the intention, and ICB leaders have tried to bully, offer phony
apologies, and claim to be ‘following orders’ as the scale of opposition
to their plans has become clear.
Only when the opposition became more vocal did the ICB reluctantly agree to
hold back on implementation and make vague promises to try “co-production”
instead of confrontation.
So who has asked for these changes?
Nobody at all. The proposals have so far only been supported by the ICB chair,
chief executive, directors, and their own immediate camp followers, while local
GPs have been furious both at the plans themselves and at the way the ICB attempted
to force them through without consultation.
GPs, patient groups and campaigners have hit back, linking up with local politicians
and MPs to organise briefings, meetings and protests.
While the ICB chiefs point to some public pressure for more speedy access to
GPs, they ignore the fact that North West London is already one of the best-performing
areas for swift access to GPs, and many local GPs already have very good levels
of accessibility.
Moreover, there has been no equivalent public pressure or campaign asking for
appointments with the much less experienced and less qualified “Additional
Roles” staff, such as Physician Associates, who would be taking most calls
under the NW London plan.
So who is driving the experiment?
The chair of NW London ICB is Penny Dash, who until 2021 was a senior partner of management consultancy McKinsey. The ICB has also brought in another major consultancy firm, KPMG to assist in rolling out their plan for complete reorganisation of primary care.
As the plan was revealed, and the growing anger of public and GPs became obvious,
various ICB leaders tried different ways to defuse the situation. Chief Executive
Rob Hurd insisted that the changes were “determined nationally”
by NHS England, leaving the ICB no scope to conduct a formal consultation.
Yet there is no national programme. Only NW London and one other ICB (Buckinghamshire,
Oxfordshire and West Berkshire) have been pushing through similar proposals.
The idea they may be implementing a national plan was cruelly shot down …
by NHS England, whose primary care director Amanda Doyle said she wanted to
“step back” – and allow local systems to get on with their
own proposals.
Hurd also claimed to be following the directions of the 2022 ‘Fuller Stocktake’
(an extensive NHS-backed report undertaken by Professor Claire Fuller): but
few of the report’s proposals have been implementedanywhere.
As that argument also fell flat, the ICB got desperate and tried to argue that
opponents of the scheme were irresponsibly frightening patients – when
in fact what was frightening them was the ICB’s plan (which is perhaps
why it was kept secret).
Unaware of the irony, the ICB’s Primary Care Director Dr Genevieve Small
told GPs:
“The bit that’s keeping me awake at night is that we have made our
patients incredibly anxious. And they have felt that general practice as they
know it is ending on the 1st April and that they won’t be able to see
their GP any more.”
This was of course what many patients DID think of the ICB plan. And there was
a simple solution: drop the plan and start talking instead to GPs and to patients
about how to generalise best practice to make services more accessible.
Since then even more evidence has emerged to confirm that NW London ICB is in
no way following rigid national instruction: NHS England has backed a project
involving seven ICBs who will test new “operating models” for GP
provision – over the next two years. It’s not clear whether any
of the models will be anything like the one at the centre of the NW London row.
But if NHS England is happy to allow an extended study like this they are clearly
not cracking the whip over North West London ICB bosses demanding they drive
through their plan for hubs.
What do the plan’s supporters want to achieve?
It appears that NWLICB’s main focus is securing a share of NHS England’s
£1.4 billion kitty for the “Additional Roles Reimbursement Scheme”,
which can be used to cover the full cost of employing 17 different types of
staff to work in primary care – but NOT to employ the staff patients most
want to see: GPs or nurses.
NHS England has stipulated that to be eligible for funding under ARRS, each
PA has to “provide a first point of contact care for patients presenting
with undifferentiated, undiagnosed problems.” (page 91)
Around the country, this has produced the ridiculous situation that fully qualified
GPs are unable to find locum and full-time posts, or are being made unemployed,
with their work being increasingly done by less qualified staff – who
are cheaper, or in many cases effectively free to employ.
Serious questions are being raised on social media about the use of PAs and other ARRS staff in single-handed GP practices – which almost by definition cannot supervise them properly – and other GP settings without adequate medical supervision.
There would have been much less opposition if NW London ICB had promised to ensure that experienced GPs would be the ones to ‘triage’ patients in each new hub, and decide which cases were sufficiently straightforward for PAs and other staff to play a useful role. Cost restraint and the substitution of GPs with PAs appear to be the main drivers of the policy.https://lowdownnhs.info/news/dash-in-to-take-charge-in-nw-london/
Afterword Youseff El-Gingihy please view slideshow... All is coming to pass!
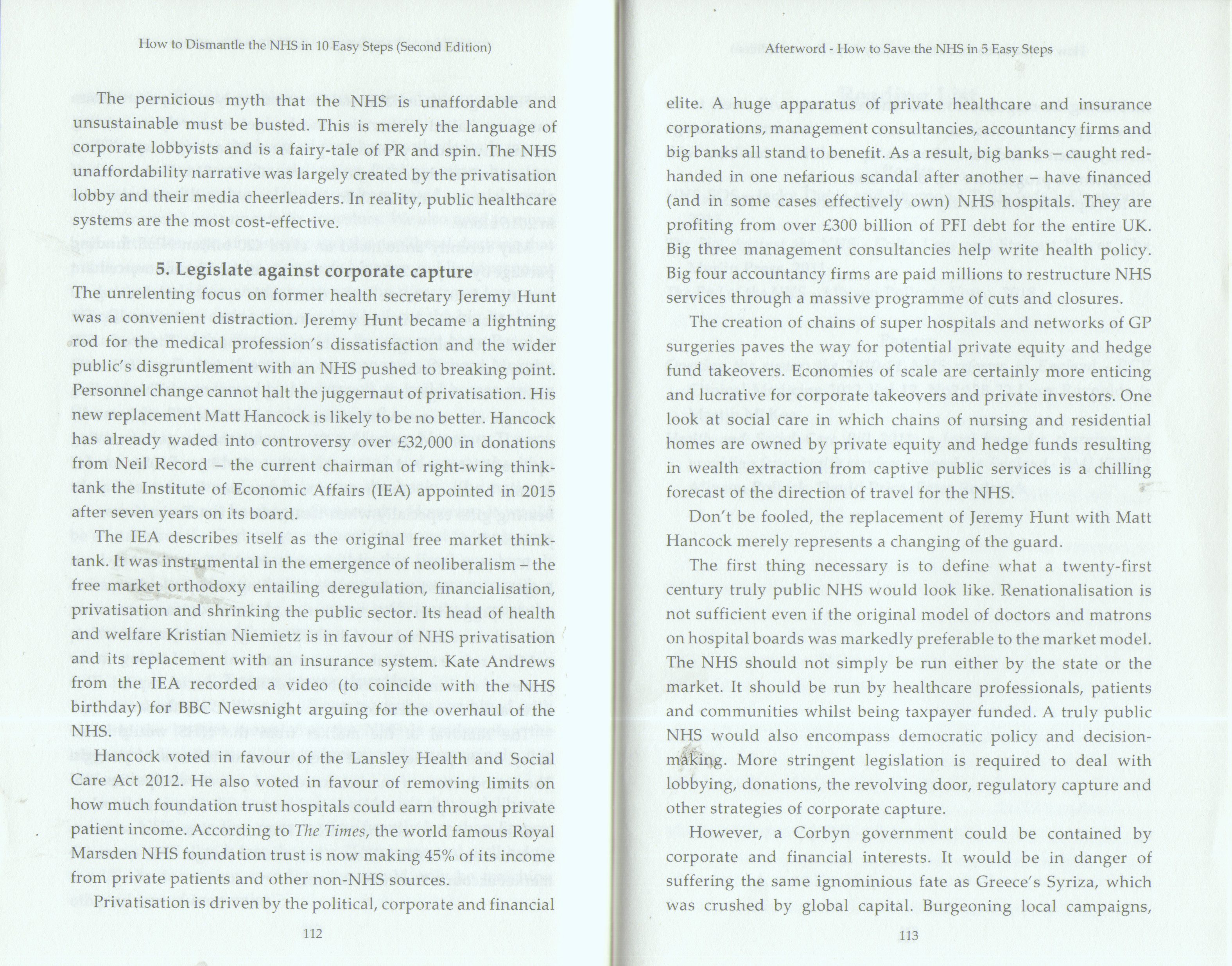
How to Dismantle the NHS in 10 Easy Steps
Profiteer private health insurers heap bribes on Health Ministers
Hancock received £32,000 donations from Neil Record-Institute of Economic Affairs
Kristian Niemietz in favour of NHS privatisation
Kate Andrew IEA argued for "overhaul" of NHS
Hancock voted for Lansley, and no limit on private work
Now atomised into private equity, big banks, insurers, consultancies McKinsey, KPMG
Finally
There is an exodus of Trust CEOs-rats leaving the sinking NHS ship...
The beginning of the NHS destruction
Labour, Tories, Lib Dems all allowed the 2012 Lansley Monster Act to go through…
fooled by 500 pages of gobbledegook, fooled by Ministers, too lazy or bigoted
to research the intent… obeying the Whips, not their common sense!
The 2021 Health (not NATIONAL) Health and SC Act-more dismantling, more outsourcing,
more privatisation- profiteers being given our taxes to profit, high CEO and
director salaries and shareholder dividends t
heir duty is to increase profits, not provide great healthcare
(Un)accountable US-style Organisations, given a large pot, allowed to ration care and keep the profits- the designed prequel to insurance pools, ready to be sold to US Insurers
Right wing Marketisers, privatisers like Hunt, Thiel, Farage, Tice all wanting to destroy the NHS and force US style insurance- high premiums, limited menus, copayments, top ups, refuse treatments, bankruptcies…
This secret plan has been undertaken under the radar
More PAs, fewer doctors, nurses, anaethetists, midwives, obstetricians, radiographers, scan readers, delays in cancer treatment…
Decimation of GP partnerships, closures, delays in access
All driven through by politicians who have private GP services, private ambulance services, private health insurance and still require the NHS to cover emergencies not covered by private insurers... matters- RTAs, strokes, covid, cardiac…
and the public never agreed all this takeover…